CONTACT A REP
Thank you!
An argenx representative will reach out to you soon, so keep an eye on your inbox!
A 26-week, multicenter, randomized, double-blind, placebo-controlled trial in 167 adult patients with gMG
PRIMARY ENDPOINT
The percentage of anti-AChR antibody positive patients who were MG-ADL responders, defined as a ≥2-point reduction in the total MG-ADL score compared to the treatment cycle baseline for at least 4 consecutive weeks during the first treatment cycle (by week 8), with the first reduction occurring no later than 1 week after the last infusion of the cycle
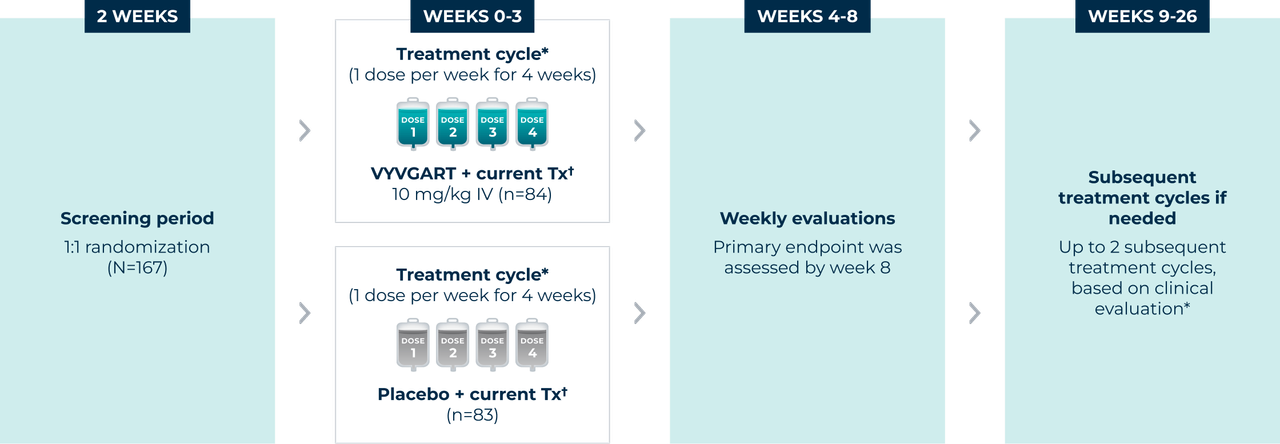
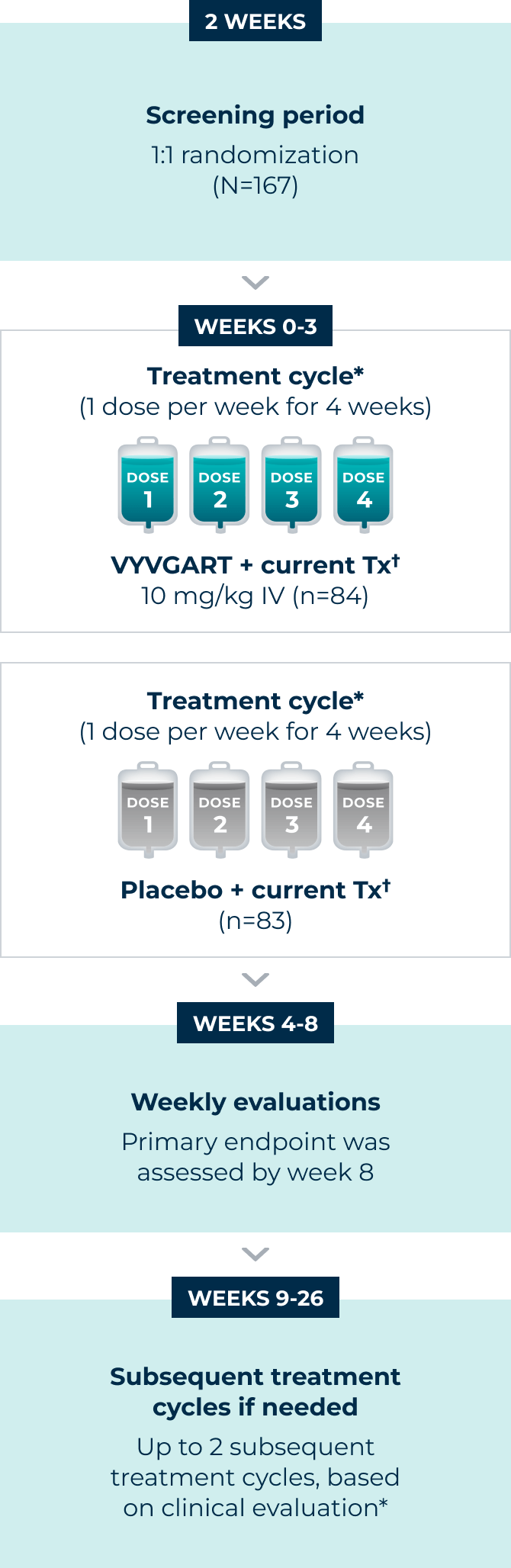
The majority of patients (n=65 for VYVGART; n=64 for placebo) were positive for AChR antibodies.†
*All patients received an initial cycle, with subsequent cycles administered based on individual clinical evaluation when their MG-ADL score was at least 5 (with >50% MG-ADL nonocular) and if the patient was an MG-ADL responder, when they no longer had a clinically meaningful decrease (defined as having a ≥2-point improvement in total MG-ADL score) compared to baseline. The minimum time between treatment cycles, specified by study protocol, was 4 weeks from the last infusion. A maximum of 3 cycles were possible in the 26-week study.
†All patients received stable doses of their current gMG treatment.
AChR=acetylcholine receptor; gMG=generalized myasthenia gravis; IV=intravenous; MG-ADL=Myasthenia Gravis Activities of Daily Living; Tx=treatment.
patients
(overall)
Mean age: 46
Female: 75%
Anti-AChR antibody
positive: n=65/84
mean baseline
(MG-ADL score;
both arms)*
MG-ADL 5-7: 24%
MG-ADL 8-9: 37%
MG-ADL ≥10: 39%
(0=normal; 24=most severe)
mean baseline
(QMG score; both arms)
Range: 4-28 (overall)
(0=normal; 39=most severe)
MGFA class at screening
Class II (Mild): 40%
Class III (Moderate): 56%
Class IV (Severe): 4%
patients
(overall)
Mean age: 48
Female: 66%
Anti-AChR antibody
positive: n=64/83
mean baseline
(MG-ADL score; both arms)*
MG-ADL 5-7: 27%†
MG-ADL 8-9: 41%†
MG-ADL ≥10: 33%†
(0=normal; 24=most severe)
mean baseline
(QMG score; both arms)
Range: 4-28 (overall)
(0=normal; 39=most severe)
MGFA class at screening
Class II (Mild): 37%
Class III (Moderate): 59%
Class IV (Severe): 4%
*MG-ADL total score of ≥5 required at screening with >50% MG-ADL nonocular.
†Conditions shown represent the 5 most prevalent comorbidities reported by investigator at baseline in the ADAPT clinical trial (N=167).
AChR=acetylcholine receptor; gMG=generalized myasthenia gravis; MG-ADL=Myasthenia Gravis Activities of Daily Living; MGFA=Myasthenia Gravis Foundation of America; NSIST=nonsteroidal immunosuppressive therapy; QMG=Quantitative Myasthenia Gravis.
A 10-week, phase 3, multicenter, randomized, open-label, parallel-group trial in 110 adult patients with gMG
PD ENDPOINT
The pharmacological effect of VYVGART Hytrulo administered subcutaneously was compared to VYVGART administered intravenously in adult patients with gMG
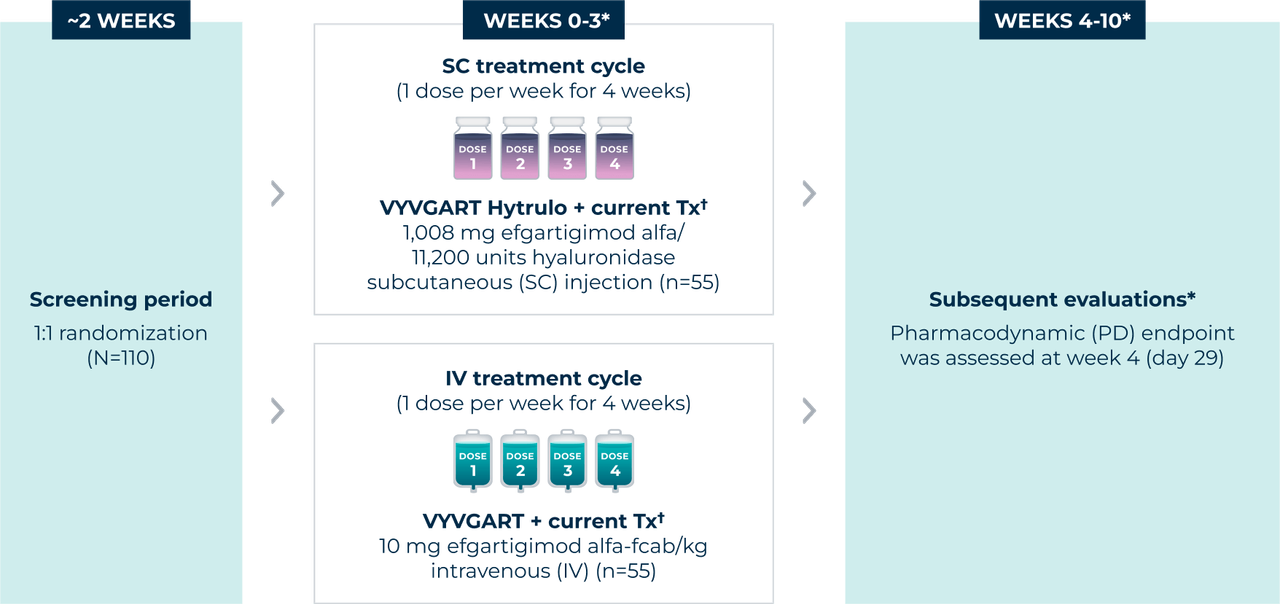
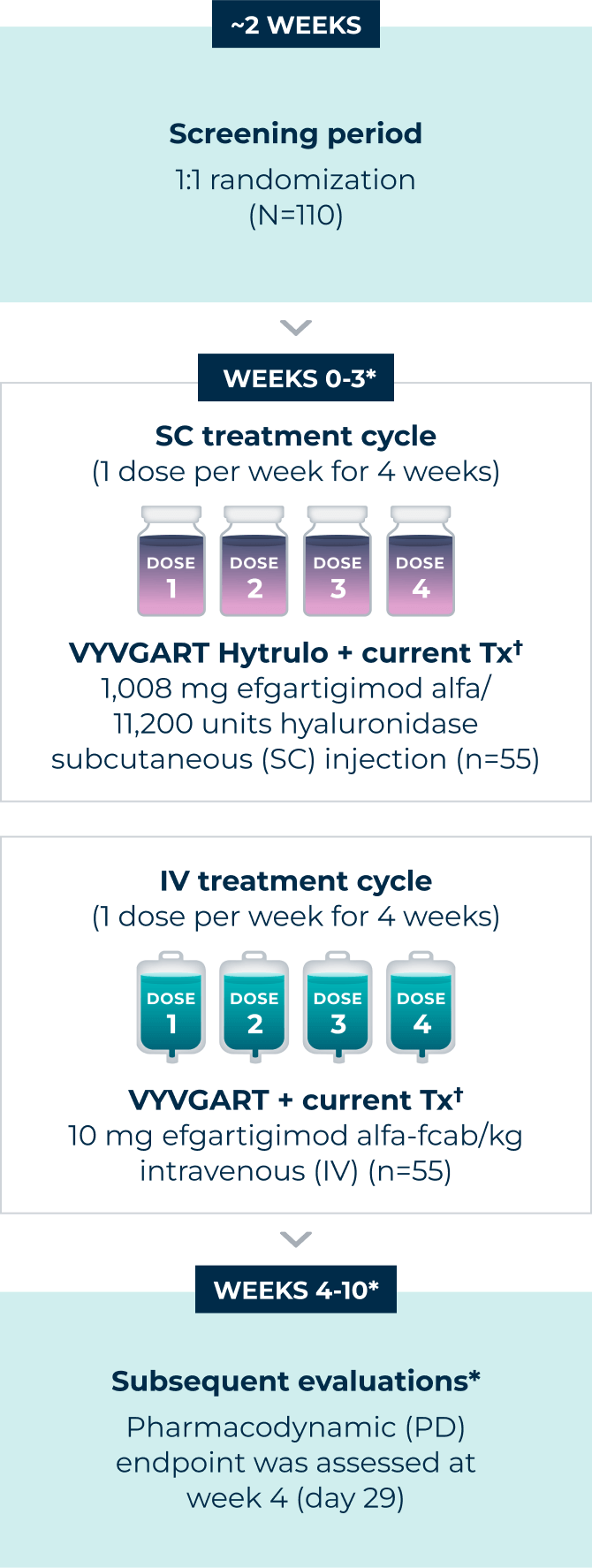
*Patients were evaluated weekly from weeks 1-8, and then at week 10.
†All patients received stable doses of their current gMG treatment.
AChR=acetylcholine receptor; gMG=generalized myasthenia gravis; MG-ADL=Myasthenia Gravis Activities of Daily Living; Tx=treatment.
patients
(overall)
Mean age: 51
Female: 56%
Anti-AChR antibody
positive: n=45/55
mean baseline
(MG-ADL score)
MG-ADL 5-7*: 36%
MG-ADL 8-9*: 29%
MG-ADL ≥10*: 35%
(0=normal; 24=most severe)
mean baseline
(QMG score)
QMG
(0=normal; 39=most severe)
MGFA class at screening
Class II (Mild): 53%†
Class III (Moderate): 44%†
Class IV (Severe): 4%†
patients
(overall)
Mean age: 56
Female: 62%
Anti-AChR antibody
positive: n=46/55
mean baseline
(MG-ADL score)
MG-ADL 5-7*: 44%†
MG-ADL 8-9*: 22%†
MG-ADL ≥10*: 35%†
(0=normal; 24=most severe)
mean baseline
(QMG score)
QMG
(0=normal; 39=most severe)
MGFA class at screening
Class II (Mild): 40%
Class III (Moderate): 55%
Class IV (Severe): 5%
*MG-ADL total score of ≥5 required at screening with >50% of the total score attributed to nonocular symptoms.
†Sum of the percentages is over 100% due to rounding.
AChR=acetylcholine receptor; gMG=generalized myasthenia gravis; MG-ADL=Myasthenia Gravis Activities of Daily Living; MGFA=Myasthenia Gravis Foundation of America; NSIST=nonsteroidal immunosuppressive therapy; QMG=Quantitative Myasthenia Gravis.
Back to Top
VYVGART HYTRULO is contraindicated in patients with serious hypersensitivity to efgartigimod alfa products, to hyaluronidase, or to any of the excipients of VYVGART HYTRULO. Reactions have included anaphylaxis and hypotension leading to syncope.
VYVGART HYTRULO may increase the risk of infection. The most common infections observed in Study 1 in patients with gMG were urinary tract infection (10% of efgartigimod alfa-fcab-treated patients vs 5% of placebo-treated patients) and respiratory tract infections (33% of efgartigimod alfa-fcab-treated patients vs 29% of placebo-treated patients). Patients on efgartigimod alfa-fcab vs placebo had below normal levels for white blood cell counts (12% vs 5%, respectively), lymphocyte counts (28% vs 19%, respectively), and neutrophil counts (13% vs 6%, respectively). The majority of infections and hematologic abnormalities were mild to moderate in severity. Delay VYVGART HYTRULO administration in patients with an active infection until the infection has resolved; monitor for clinical signs and symptoms of infections. If serious infection occurs, administer appropriate treatment and consider withholding VYVGART HYTRULO until the infection has resolved.
Evaluate the need to administer age-appropriate vaccines according to immunization guidelines before initiation of a new treatment cycle with VYVGART HYTRULO. The safety of immunization with live vaccines and the immune response to vaccination during treatment with VYVGART HYTRULO are unknown. Because VYVGART HYTRULO causes a reduction in immunoglobulin G (IgG) levels, vaccination with live vaccines is not recommended during treatment with VYVGART HYTRULO.
In clinical trials, hypersensitivity reactions, including rash, angioedema, and dyspnea were observed in patients treated with VYVGART HYTRULO or intravenous efgartigimod alfa-fcab. Urticaria was also observed in patients treated with VYVGART HYTRULO. Hypersensitivity reactions were mild or moderate, occurred within 1 hour to 3 weeks of administration. Anaphylaxis and hypotension leading to syncope have been reported in postmarketing experience with intravenous efgartigimod alfa-fcab. Anaphylaxis and hypotension occurred during or within an hour of administration and led to infusion discontinuation and in some cases to permanent treatment discontinuation. Monitor for clinical signs and symptoms of hypersensitivity reactions for at least 30 minutes after administration. If a hypersensitivity reaction occurs, the healthcare professional should institute appropriate measures if needed or the patient should seek medical attention.
Infusion-related reactions have been reported with intravenous efgartigimod alfa-fcab in postmarketing experience. The most frequent symptoms and signs were hypertension, chills, shivering, and thoracic, abdominal, and back pain. Infusion-related reactions occurred during or within an hour of administration and led to infusion discontinuation. If a severe infusion/injection-related reaction occurs, initiate appropriate therapy. Consider the risks and benefits of readministering VYVGART HYTRULO following a severe infusion/injection-related reaction. If a mild to moderate infusion/injection-related reaction occurs, patients may be rechallenged with close clinical observation, slower infusion/injection rates, and pre-medications.
Patients with gMG: In Study 1, the most common (≥10%) adverse reactions in efgartigimod alfa-fcab-treated patients were respiratory tract infection, headache, and urinary tract infection. In Study 2, the most common (≥10%) adverse reactions in VYVGART HYTRULO-treated patients were injection site reactions and headache. Injection site reactions occurred in 38% of VYVGART HYTRULO-treated patients, including injection site rash, erythema, pruritus, bruising, pain, and urticaria. In Study 2 and its open-label extension in patients with gMG, all injection site reactions were mild to moderate in severity and did not lead to treatment discontinuation. The majority occurred within 24 hours after administration and resolved spontaneously. Most injection site reactions occurred during the first treatment cycle, and the incidence decreased with each subsequent cycle.
Patients with CIDP: In Study 3 stage B, the overall safety profile observed in patients with CIDP treated with VYVGART HYTRULO was consistent with the known safety profile of VYVGART HYTRULO and of efgartigimod alfa-fcab administered intravenously. In Study 3, injection site reactions occurred in 15% of patients treated with VYVGART HYTRULO compared to 6% of patients who received placebo. The most common of these injection site reactions were injection site bruising and injection site erythema. All injection site reactions were mild to moderate in severity. Most injection site reactions occurred during the first 3 months of treatment.
As VYVGART HYTRULO is expected to reduce maternal IgG antibody levels, reduction in passive protection to the newborn is anticipated. Risk and benefits should be considered prior to administering live vaccines to infants exposed to VYVGART HYTRULO in utero.
There is no information regarding the presence of efgartigimod alfa or hyaluronidase, from administration of VYVGART HYTRULO, in human milk, the effects on the breastfed infant, or the effects on milk production. Maternal IgG is known to be present in human milk. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for VYVGART HYTRULO and any potential adverse effects on the breastfed infant from VYVGART HYTRULO or from the underlying maternal condition.
VYVGART HYTRULO® (efgartigimod alfa and hyaluronidase-qvfc) is indicated for the treatment of adult patients with generalized myasthenia gravis (gMG) who are anti-acetylcholine receptor (AChR) antibody positive.
VYVGART HYTRULO® (efgartigimod alfa and hyaluronidase-qvfc) is indicated for the treatment of adult patients with chronic inflammatory demyelinating polyneuropathy (CIDP).
Please see the full Prescribing Information.
You may report side effects to the US Food and Drug Administration by visiting http://www.fda.gov/medwatch or calling 1-800-FDA-1088. You may also report side effects to argenx US, Inc, at 1-833-argx411 (1-833-274-9411).
Dosage Forms and Strengths: VYVGART Hytrulo is available as a single-dose subcutaneous injection containing: 200 mg/mL of efgartigimod alfa and 2,000 U/mL of hyaluronidase per prefilled syringe, or 180 mg/mL of efgartigimod alfa and 2,000 U/mL of hyaluronidase per vial.
VYVGART is contraindicated in patients with serious hypersensitivity to efgartigimod alfa products or to any of the excipients of VYVGART. Reactions have included anaphylaxis and hypotension leading to syncope.
VYVGART may increase the risk of infection. The most common infections observed in Study 1 were urinary tract infection (10% for VYVGART vs 5% for placebo) and respiratory tract infections (33% for VYVGART vs 29% for placebo). Patients on VYVGART vs placebo had below normal levels for white blood cell counts (12% vs 5%, respectively), lymphocyte counts (28% vs 19%, respectively), and neutrophil counts (13% vs 6%, respectively). The majority of infections and hematologic abnormalities were mild to moderate in severity. Delay VYVGART administration in patients with an active infection until the infection has resolved; monitor for clinical signs and symptoms of infections. If serious infection occurs, administer appropriate treatment and consider withholding VYVGART until the infection has resolved.
Evaluate the need to administer age-appropriate vaccines according to immunization guidelines before initiation of a new treatment cycle with VYVGART. The safety of immunization with live vaccines and the immune response to vaccination during treatment with VYVGART are unknown. Because VYVGART causes a reduction in immunoglobulin G (IgG) levels, vaccination with live vaccines is not recommended during treatment with VYVGART.
In clinical trials, hypersensitivity reactions, including rash, angioedema, and dyspnea were observed in VYVGART-treated patients. Hypersensitivity reactions were mild or moderate, occurred within 1 hour to 3 weeks of administration, and did not lead to treatment discontinuation. Anaphylaxis and hypotension leading to syncope have been reported in postmarketing experience with VYVGART. Anaphylaxis and hypotension occurred during or within an hour of administration and led to infusion discontinuation and in some cases to permanent treatment discontinuation. Monitor patients during administration and for 1 hour thereafter for clinical signs and symptoms of hypersensitivity reactions. If a hypersensitivity reaction occurs, the healthcare professional should institute appropriate measures if needed or the patient should seek medical attention.
Infusion-related reactions have been reported with VYVGART in postmarketing experience. The most frequent symptoms and signs were hypertension, chills, shivering, and thoracic, abdominal, and back pain. Infusion-related reactions occurred during or within an hour of administration and led to infusion discontinuation. If a severe infusion-related reaction occurs during administration, discontinue VYVGART infusion and initiate appropriate therapy. Consider the risks and benefits of readministering VYVGART following a severe infusion-related reaction. If a mild to moderate infusion-related reaction occurs, patients may be rechallenged with close clinical observation, slower infusion rates, and pre-medications.
In Study 1, the most common (≥10%) adverse reactions with VYVGART were respiratory tract infection, headache, and urinary tract infection.
As VYVGART is expected to reduce maternal IgG antibody levels, reduction in passive protection to the newborn is anticipated. Risk and benefits should be considered prior to administering live vaccines to infants exposed to VYVGART in utero.
There is no information regarding the presence of efgartigimod alfa-fcab in human milk, the effects on the breastfed infant, or the effects on milk production. Maternal IgG is known to be present in human milk. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for VYVGART and any potential adverse effects on the breastfed infant from VYVGART or from the underlying maternal condition.
VYVGART® (efgartigimod alfa-fcab) is indicated for the treatment of generalized myasthenia gravis in adult patients who are anti-acetylcholine receptor (AChR) antibody positive.
Please see the full Prescribing Information.
You may report side effects to the US Food and Drug Administration by visiting http://www.fda.gov/medwatch or calling 1-800-FDA-1088. You may also report side effects to argenx US, Inc, at 1-833-argx411 (1-833-274-9411).
Dosage Form and Strength: VYVGART is available as a single-dose injection for intravenous use containing 400 mg/20 mL of efgartigimod alfa-fcab per vial.
VYVGART HYTRULO is contraindicated in patients with serious hypersensitivity to efgartigimod alfa products, to hyaluronidase, or to any of the excipients of VYVGART HYTRULO. Reactions have included anaphylaxis and hypotension leading to syncope.
VYVGART HYTRULO may increase the risk of infection. The most common infections observed in Study 1 in patients with gMG were urinary tract infection (10% of efgartigimod alfa-fcab-treated patients vs 5% of placebo-treated patients) and respiratory tract infections (33% of efgartigimod alfa-fcab-treated patients vs 29% of placebo-treated patients). Patients on efgartigimod alfa-fcab vs placebo had below normal levels for white blood cell counts (12% vs 5%, respectively), lymphocyte counts (28% vs 19%, respectively), and neutrophil counts (13% vs 6%, respectively). The majority of infections and hematologic abnormalities were mild to moderate in severity. Delay VYVGART HYTRULO administration in patients with an active infection until the infection has resolved; monitor for clinical signs and symptoms of infections. If serious infection occurs, administer appropriate treatment and consider withholding VYVGART HYTRULO until the infection has resolved.
Evaluate the need to administer age-appropriate vaccines according to immunization guidelines before initiation of a new treatment cycle with VYVGART HYTRULO. The safety of immunization with live vaccines and the immune response to vaccination during treatment with VYVGART HYTRULO are unknown. Because VYVGART HYTRULO causes a reduction in immunoglobulin G (IgG) levels, vaccination with live vaccines is not recommended during treatment with VYVGART HYTRULO.
In clinical trials, hypersensitivity reactions, including rash, angioedema, and dyspnea were observed in patients treated with VYVGART HYTRULO or intravenous efgartigimod alfa-fcab. Urticaria was also observed in patients treated with VYVGART HYTRULO. Hypersensitivity reactions were mild or moderate, occurred within 1 hour to 3 weeks of administration. Anaphylaxis and hypotension leading to syncope have been reported in postmarketing experience with intravenous efgartigimod alfa-fcab. Anaphylaxis and hypotension occurred during or within an hour of administration and led to infusion discontinuation and in some cases to permanent treatment discontinuation. Monitor for clinical signs and symptoms of hypersensitivity reactions for at least 30 minutes after administration. If a hypersensitivity reaction occurs, the healthcare professional should institute appropriate measures if needed or the patient should seek medical attention.
Infusion-related reactions have been reported with intravenous efgartigimod alfa-fcab in postmarketing experience. The most frequent symptoms and signs were hypertension, chills, shivering, and thoracic, abdominal, and back pain. Infusion-related reactions occurred during or within an hour of administration and led to infusion discontinuation. If a severe infusion/injection-related reaction occurs, initiate appropriate therapy. Consider the risks and benefits of readministering VYVGART HYTRULO following a severe infusion/injection-related reaction. If a mild to moderate infusion/injection-related reaction occurs, patients may be rechallenged with close clinical observation, slower infusion/injection rates, and pre-medications.
Patients with gMG: In Study 1, the most common (≥10%) adverse reactions in efgartigimod alfa-fcab-treated patients were respiratory tract infection, headache, and urinary tract infection. In Study 2, the most common (≥10%) adverse reactions in VYVGART HYTRULO-treated patients were injection site reactions and headache. Injection site reactions occurred in 38% of VYVGART HYTRULO-treated patients, including injection site rash, erythema, pruritus, bruising, pain, and urticaria. In Study 2 and its open-label extension in patients with gMG, all injection site reactions were mild to moderate in severity and did not lead to treatment discontinuation. The majority occurred within 24 hours after administration and resolved spontaneously. Most injection site reactions occurred during the first treatment cycle, and the incidence decreased with each subsequent cycle.
Patients with CIDP: In Study 3 stage B, the overall safety profile observed in patients with CIDP treated with VYVGART HYTRULO was consistent with the known safety profile of VYVGART HYTRULO and of efgartigimod alfa-fcab administered intravenously. In Study 3, injection site reactions occurred in 15% of patients treated with VYVGART HYTRULO compared to 6% of patients who received placebo. The most common of these injection site reactions were injection site bruising and injection site erythema. All injection site reactions were mild to moderate in severity. Most injection site reactions occurred during the first 3 months of treatment.
As VYVGART HYTRULO is expected to reduce maternal IgG antibody levels, reduction in passive protection to the newborn is anticipated. Risk and benefits should be considered prior to administering live vaccines to infants exposed to VYVGART HYTRULO in utero.
There is no information regarding the presence of efgartigimod alfa or hyaluronidase, from administration of VYVGART HYTRULO, in human milk, the effects on the breastfed infant, or the effects on milk production. Maternal IgG is known to be present in human milk. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for VYVGART HYTRULO and any potential adverse effects on the breastfed infant from VYVGART HYTRULO or from the underlying maternal condition.
VYVGART HYTRULO® (efgartigimod alfa and hyaluronidase-qvfc) is indicated for the treatment of adult patients with generalized myasthenia gravis (gMG) who are anti-acetylcholine receptor (AChR) antibody positive.
VYVGART HYTRULO® (efgartigimod alfa and hyaluronidase-qvfc) is indicated for the treatment of adult patients with chronic inflammatory demyelinating polyneuropathy (CIDP).
Please see the full Prescribing Information.
You may report side effects to the US Food and Drug Administration by visiting http://www.fda.gov/medwatch or calling 1-800-FDA-1088. You may also report side effects to argenx US, Inc, at 1-833-argx411 (1-833-274-9411).
Dosage Forms and Strengths: VYVGART Hytrulo is available as a single-dose subcutaneous injection containing: 200 mg/mL of efgartigimod alfa and 2,000 U/mL of hyaluronidase per prefilled syringe, or 180 mg/mL of efgartigimod alfa and 2,000 U/mL of hyaluronidase per vial.
VYVGART is contraindicated in patients with serious hypersensitivity to efgartigimod alfa products or to any of the excipients of VYVGART. Reactions have included anaphylaxis and hypotension leading to syncope.
VYVGART may increase the risk of infection. The most common infections observed in Study 1 were urinary tract infection (10% for VYVGART vs 5% for placebo) and respiratory tract infections (33% for VYVGART vs 29% for placebo). Patients on VYVGART vs placebo had below normal levels for white blood cell counts (12% vs 5%, respectively), lymphocyte counts (28% vs 19%, respectively), and neutrophil counts (13% vs 6%, respectively). The majority of infections and hematologic abnormalities were mild to moderate in severity. Delay VYVGART administration in patients with an active infection until the infection has resolved; monitor for clinical signs and symptoms of infections. If serious infection occurs, administer appropriate treatment and consider withholding VYVGART until the infection has resolved.
Evaluate the need to administer age-appropriate vaccines according to immunization guidelines before initiation of a new treatment cycle with VYVGART. The safety of immunization with live vaccines and the immune response to vaccination during treatment with VYVGART are unknown. Because VYVGART causes a reduction in immunoglobulin G (IgG) levels, vaccination with live vaccines is not recommended during treatment with VYVGART.
In clinical trials, hypersensitivity reactions, including rash, angioedema, and dyspnea were observed in VYVGART-treated patients. Hypersensitivity reactions were mild or moderate, occurred within 1 hour to 3 weeks of administration, and did not lead to treatment discontinuation. Anaphylaxis and hypotension leading to syncope have been reported in postmarketing experience with VYVGART. Anaphylaxis and hypotension occurred during or within an hour of administration and led to infusion discontinuation and in some cases to permanent treatment discontinuation. Monitor patients during administration and for 1 hour thereafter for clinical signs and symptoms of hypersensitivity reactions. If a hypersensitivity reaction occurs, the healthcare professional should institute appropriate measures if needed or the patient should seek medical attention.
Infusion-related reactions have been reported with VYVGART in postmarketing experience. The most frequent symptoms and signs were hypertension, chills, shivering, and thoracic, abdominal, and back pain. Infusion-related reactions occurred during or within an hour of administration and led to infusion discontinuation. If a severe infusion-related reaction occurs during administration, discontinue VYVGART infusion and initiate appropriate therapy. Consider the risks and benefits of readministering VYVGART following a severe infusion-related reaction. If a mild to moderate infusion-related reaction occurs, patients may be rechallenged with close clinical observation, slower infusion rates, and pre-medications.
Study 1, the most common (≥10%) adverse reactions with VYVGART were respiratory tract infection, headache, and urinary tract infection.
As VYVGART is expected to reduce maternal IgG antibody levels, reduction in passive protection to the newborn is anticipated. Risk and benefits should be considered prior to administering live vaccines to infants exposed to VYVGART in utero.
There is no information regarding the presence of efgartigimod alfa-fcab in human milk, the effects on the breastfed infant, or the effects on milk production. Maternal IgG is known to be present in human milk. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for VYVGART and any potential adverse effects on the breastfed infant from VYVGART or from the underlying maternal condition.
VYVGART® (efgartigimod alfa-fcab) is indicated for the treatment of generalized myasthenia gravis in adult patients who are anti-acetylcholine receptor (AChR) antibody positive.
Please see the full Prescribing Information.
You may report side effects to the US Food and Drug Administration by visiting http://www.fda.gov/medwatch or calling 1-800-FDA-1088. You may also report side effects to argenx US, Inc, at 1-833-argx411 (1-833-274-9411).
Dosage Form and Strength: VYVGART is available as a single-dose injection for intravenous use containing 400 mg/20 mL of efgartigimod alfa-fcab per vial.
References: 1. VYVGART. Prescribing information. argenx US Inc; 2025. 2. Howard JF Jr et al. Lancet Neurol. 2021;20(7):526-536. doi:10.1016/S1474-4422(21)00159-9 3. Data on file. REF-00690. argenx US Inc. November 2021. 4. Data on file. REF-00692. argenx US Inc. November 2021. 5. Howard JF Jr et al. Neurotherapeutics. 2024;21(5):1-12. doi:10.1016/j.neurot.2024.e00378 6. VYVGART Hytrulo. Prescribing information. argenx US Inc; 2025. 7. Data on file. REF-01893. argenx US Inc. June 2023.
